Conditions: Subglottic Stenosis and Tracheal Stenosis
what are subglottic stenosis, tracheal stenosis?
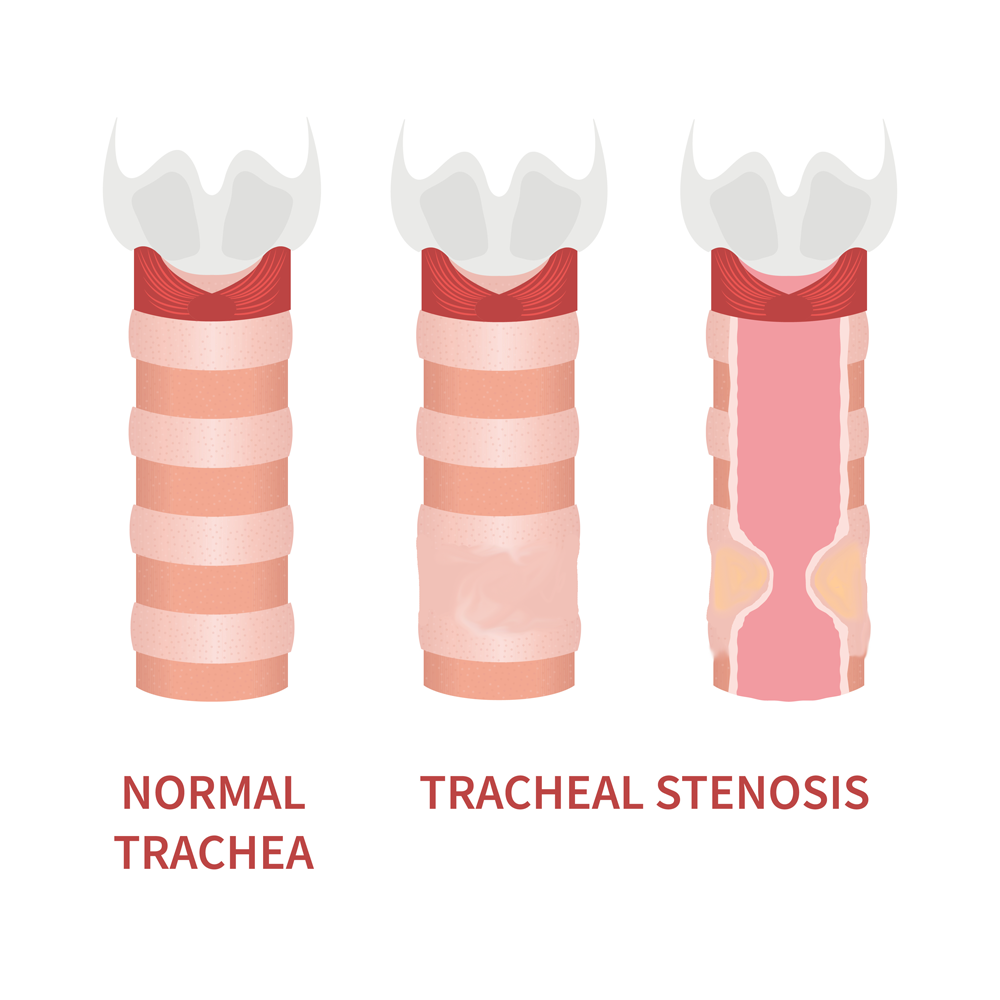
Stenosis means narrowing.
Subglottic means below the vocal cords (glottis).
Subglottic stenosis refers to abnormal narrowing of airway a short distance below the level of the vocal cords.
Laryngeal stenosis refers to abnormal narrowing of the larynx, which is a cartilage framework that houses the vocal cords.
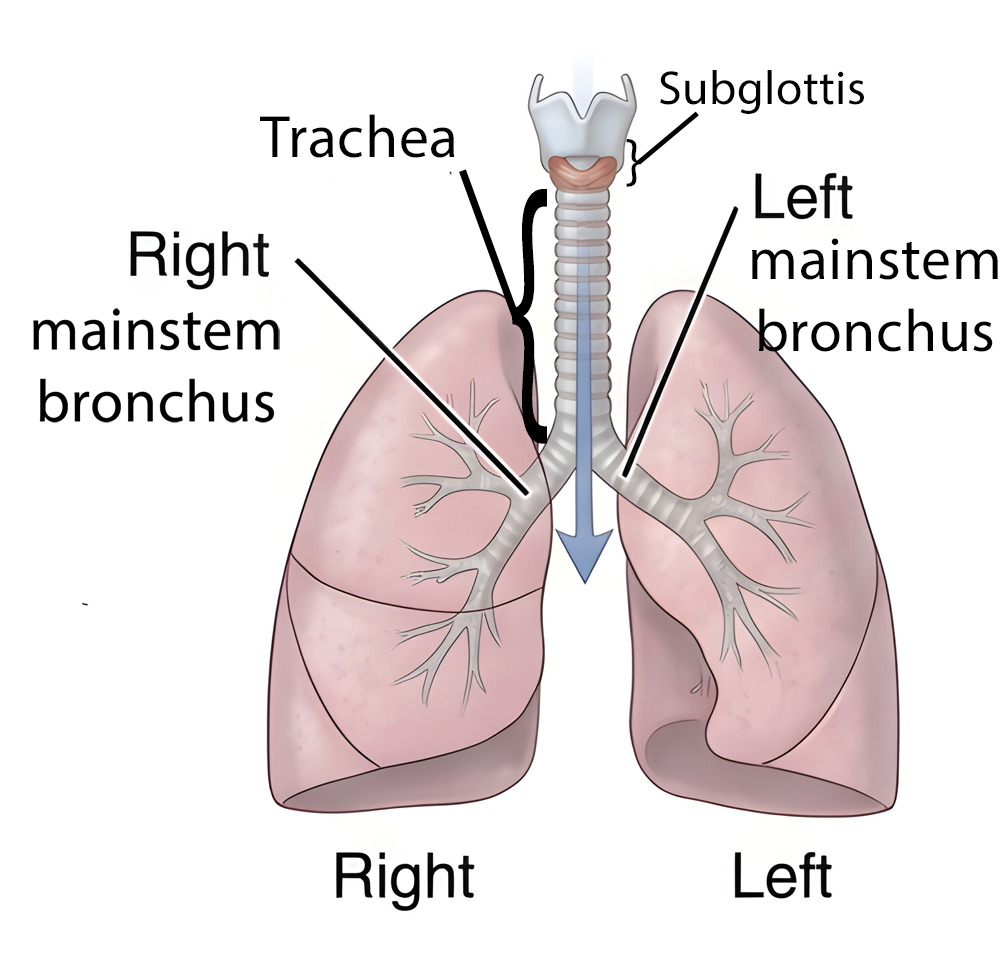
Tracheal stenosis refers to abnormal narrowing of the trachea,
Laryngeaal, subglottic and tracheal stenosis may overlap simultaneously, and the causes and treatments are similar for each. Laryngotracheal stenosis is a narrowing from the vocal cords down to the trachea.
what are the symptoms of subglottic stenosis?
The most common symptom of stenosis of the larynx, subglottis, or trachea is breathlessness (dyspnea) particularly when undertaking physical activities requiring some exertion. Since these types of airway stenosis develop gradually, the symptom of breathlessness typically occur gradually as well. An affected individual may also experience added respiratory sounds (stridor), though mild stridor may sometimes be mistaken for a wheeze. This overlap in presentation between mild stridor and wheezing creates a diagnostic pitfall in which some patients with subglottic stenosis are initially incorrectly diagnosed and treated as having asthma.
what causes subglottic stenosis?
The most common cause of subglottic stenosis (SGS) in adults is prolonged endotracheal intubation, which accounts for the majority of acquired cases. Beyond this, the etiologies can be broadly classified as acquired (far more common) and congenital (rare).
Acquired Causes
• Prolonged or traumatic intubation — This can occur when an endotracheal breathing tube exerts pressure on the subglottic/tracheal lining (mucosa), leading to lack of blood flow, tissue death, then swelling, ulceration and ultimately fibrotic scar formation. Post-intubation subglottic develops in approximately 0.9%–8.3% of intubated neonates, and risk increases with duration of intubation, oversized tubes, multiple intubation attempts, and inadequate sedation. Symptoms typically present 4–6 weeks after the acute injury.
• Idiopathic subglottic stenosis (iSGS) — Accounts for roughly 15%–30% of cases and presents almost exclusively in middle-aged white females. It is a chronic fibroinflammatory condition with no identifiable precipitant. Proposed contributing mechanisms include estrogen-mediated effects, laryngopharyngeal reflux, and aberrant wound healing. Some investigators have suggested iSGS may represent a spectrum of autoimmune-mediated disease.
• Autoimmune and inflammatory diseases — Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis and relapsing polychondritis (RP) are the two most common inflammatory causes. In one multicenter study, GPA accounted for 41% and RP for 26% of non-traumatic, non-tumoral SGS/tracheal stenosis cases. Other inflammatory etiologies include sarcoidosis, amyloidosis, bullous dermatoses, and Crohn's disease.
• Other acquired causes — Tracheostomy and cricothyroidotomy, external laryngeal trauma, chemical or thermal inhalation injury, chondroradionecrosis after radiation therapy, and gastroesophageal reflux disease.
Congenital Causes (present at birth)
Congenital SGS is rare and results from an abnormally small cricoid cartilage. It is the third most common congenital laryngeal anomaly in children.
Key Clinical Considerations
Distinguishing between iSGS and GPA-associated SGS can be diagnostically challenging, particularly when SGS is the presenting symptom of GPA — SGS was the initial disease manifestation in 66% of inflammatory cases in one published series. GPA-related stenoses tend to be circumferential and subglottic, while RP-related stenoses are more often anterior, tracheal, calcified, and extend to the bronchi. Comorbidities such as obesity and diabetes mellitus are frequently observed in patients with acquired SGS and may influence disease severity and recurrence.
how is subglottic stenosis diagnosed?
Clinical Presentation
Patients typically present with progressive dyspnea, noisy breathing (stridor) that occurs with both inhalation and exhalation (biphasic), chronic cough, exercise intolerance, and voice changes. Symptoms depend on the degree of narrowing — mild stenosis (grades 1–2) may be asymptomatic or present only with recurrent upper respiratory infections, while severe stenosis (grades 3–4) causes stridor, respiratory distress, and feeding difficulties in children. The diagnosis is often delayed or considered after other possibilities given its rarity.
Diagnostic Modalities
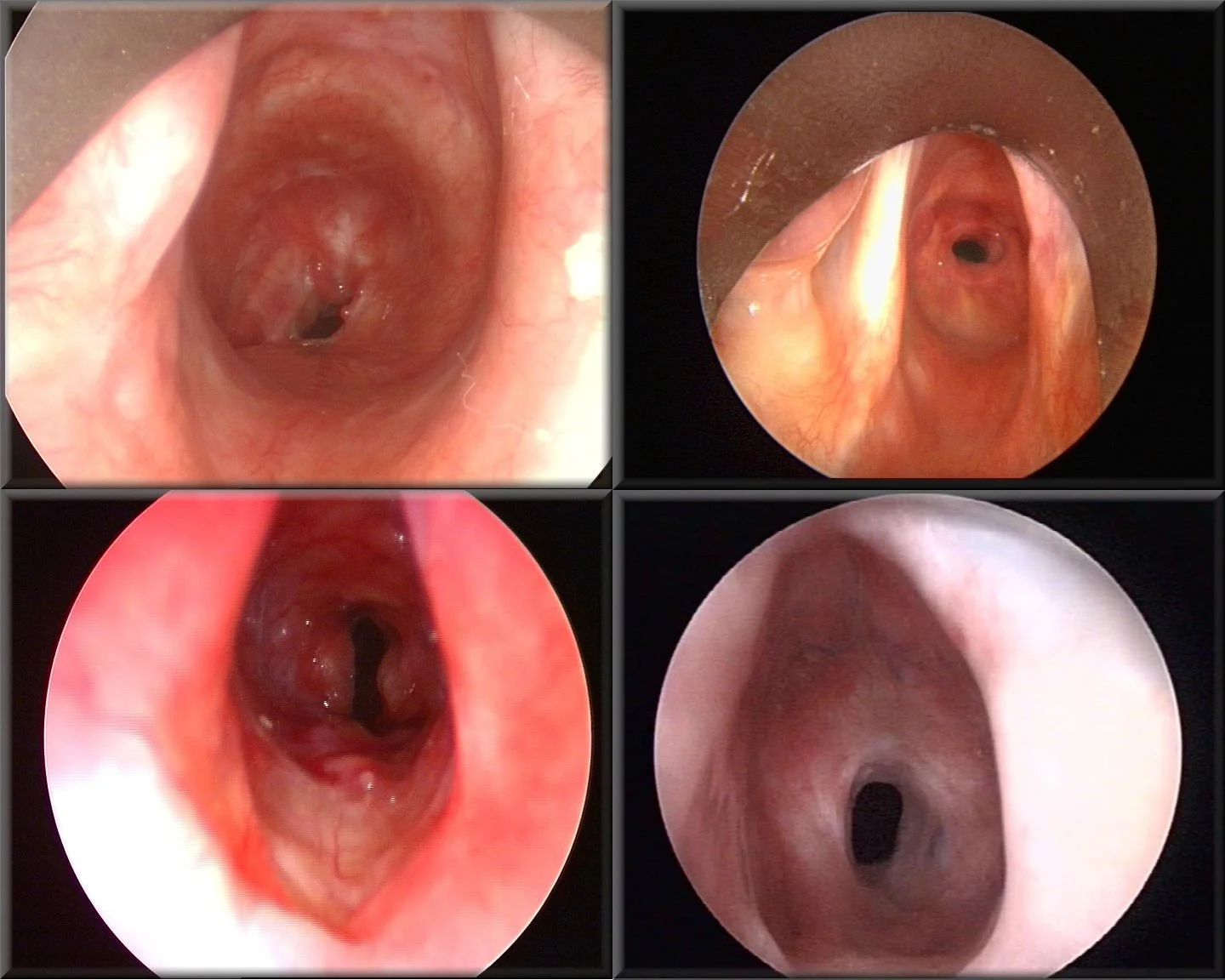
Examples of subglottic stenosis, as viewed from above the vocal cords. The white(ish) structures on the sides of each image are the vocal cords. The narrowing of the airway below this level is visible as the small black passageway. Image Source: Rn cantab, CC BY-SA 3.0 <https://creativecommons.org/licenses/by-sa/3.0>, via Wikimedia Commons
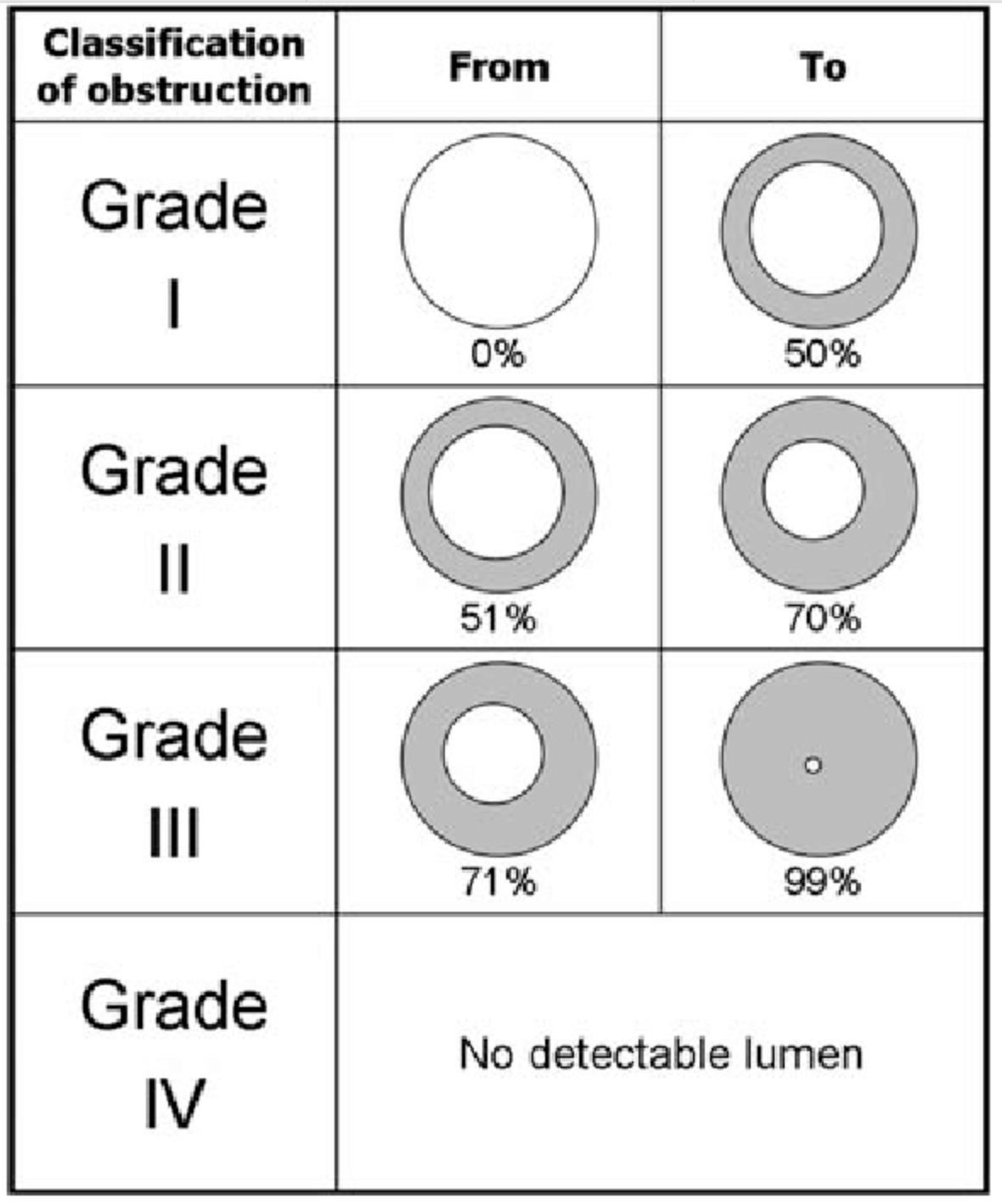
Meyer-Cotton grading scale for severity of subglottic stenosis
Flexible laryngoscopy (awake): Evaluates the upper airway and can sometimes identify subglottic narrowing in the office setting, though the view may be limited.
Direct laryngoscopy and bronchoscopy: The gold standard for definitive diagnosis. Allows direct visualization, grading of stenosis severity, and tissue biopsy when needed. The Myer-Cotton grading scale is the most commonly used classification system, based on the percentage of luminal obstruction: Grade 1 (<50%), Grade 2 (51–70%), Grade 3 (71–99%), Grade 4 (complete obstruction).
CT imaging with multiplanar reconstruction: Highly accurate for detecting laryngotracheal stenosis and provides information on stenosis length, location, and extraluminal disease. Virtual endoscopy can supplement direct visualization. CT can also evaluate airway dynamics during inspiration and expiration.
Pulmonary function testing (PFTs): Useful for surveillance and differentiating upper from lower airway obstruction. The flow-volume loop may show characteristic flattening. The expiratory disproportion index (EDI) has been described as a sensitive and specific tool for differentiating laryngotracheal stenosis from conditions like asthma or COPD.
Laboratory testing: Important to evaluate for autoimmune etiologies such as granulomatosis with polyangiitis (GPA) or relapsing polychondritis, which can cause SGS. ANCA testing and inflammatory markers are usually obtained when an autoimmune cause is suspected.
Biopsy/pathology: Tissue sampling during endoscopy helps distinguish between idiopathic, autoimmune, and other causes.
how is subglottic stenosis treated?
Identification of the cause, when possible, allows for treatment of the predisposing condition.
Placement of a tracheostomy tube may be necessary to secure the airway prior to any attempt to treat the stenosis. Removal of the tracheostomy tube is a goal, but not a guarantee.
One or more of the following surgical treatment options may be applied to treatment of a specific subglottic stenosis situation:
Tracheal dilation (stretching the narrow segment)
Making partial thickness relaxing cuts in the internal aspect of the narrow segment. This may be done with a knife or a laser.
Injecting or applying a medicine to the treated area (such as a steroid and/or mitomycin-C) to reduce the risk of recurrence
Stenting of the narrow segment to provide structure and resistance to narrowing
Removing (resecting) the narrow segment and connecting the two ends of trachea
Opening the narrow segment and inserting a spacer (stent) to add width to the narrow segment
Can subglottic stenosis recur after treatment?
Yes. Subglottic stenosis can recur after treatment, though the risk and pattern of recurrence depend on the cause, severity, and the treatment method used.
Causes: Acquired subglottic stenosis (most commonly from prolonged intubation, infection, trauma, autoimmune disease, or reflux) and congenital stenosis behave differently. Inflammatory or ongoing disease processes (e.g., granulomatosis with polyangiitis, relapsing polychondritis) carry higher recurrence risk unless the underlying disease is controlled.
Treatment types and recurrence risk:
Endoscopic procedures (dilation, endoscopic excision, laser, steroid injections): less invasive, good for short, web-like or immature scars, but have relatively higher recurrence rates and often require repeated procedures.
Open surgical reconstruction (laryngotracheal reconstruction with cartilage grafting, cricotracheal resection): more definitive for longer or mature strictures and generally have lower recurrence rates when performed at experienced centers.
Tracheostomy: relieves airway obstruction by bypassing it but does not treat the stenosis; dependence can be permanent and recurrence of stenosis at or below the tracheostomy site is possible.
Timing: Recurrence can occur early (weeks to months) if scar tissue reforms or if the underlying cause remains active, or late (months to years) particularly if progressive disease is present.
Predictors of recurrence:
Severity and length of the stenosis
Presence of active inflammatory or autoimmune disease
Prior radiation or severe infection
Ongoing gastroesophageal reflux or aspiration
Ongoing drivers of subglottic stenosis (e.g., continued intubation with a breathing tube, uncontrolled autoimmune disease)
Management of recurrence: Repeat endoscopic treatment for short recurrences; consider definitive open reconstruction if repeated endoscopic procedures fail or if stenosis is extensive. Treat underlying disease (immunosuppression for autoimmune conditions, control reflux, stop injurious exposures).
Prognosis: Many patients achieve durable airway patency after appropriate surgery and medical management, especially when the underlying cause is treated. Some patients require multiple interventions or long-term surveillance.

HOW TO GET THE MOST FROM YOUR APPOINTMENT
Appointment time is valuable. Below are some suggestions to make the most of your appointment. This preparation will help you and your doctor maximize efficiency and accuracy, freeing up time for questions and answers.
• Click here to prepare for your neck mass/swelling/lump appointment.