Diagnostics: SPECT (single positron emission computed tomography) scan
What is a SPECT-CT SCAN?

SPECT-CT (Single-Photon Emission Computed Tomography/Computed Tomography) is a hybrid imaging modality that combines the functional information from SPECT with the anatomical detail from CT in a single imaging session.
How it works: SPECT uses gamma-emitting radiopharmaceuticals to detect physiological processes (e.g., blood flow, receptor expression, bone metabolism), while CT provides high-resolution structural images. Both datasets are acquired sequentially with the patient in the same position, allowing precise co-registration and generation of fused images. The following figure illustrates the two main hardware configurations — a sequential dual-gantry system and a compact single-gantry design:
What are the clinical applications of SPECT-CT?
Common clinical applications include myocardial perfusion imaging (cardiac SPECT/CT), bone scintigraphy, parathyroid localization for hyperparathyroidism, sentinel lymph node mapping, thyroid cancer imaging with radioiodine, somatostatin receptor scintigraphy for neuroendocrine tumors, and infection imaging.
How is a SPECT-CT used to locate parathyroid adenomas?
The American College of Radiology (ACR) Appropriateness Criteria recommends Tc-99m sestamibi SPECT/CT as a well-established first-line imaging modality for preoperative localization of parathyroid adenomas in primary hyperparathyroidism.
Imaging protocols: Two main scintigraphic approaches incorporate SPECT/CT:
Dual-phase single-tracer (sestamibi only): Tc-99m sestamibi is injected, and planar images are acquired at early (10–30 min) and delayed (90–180 min) timepoints. SPECT or SPECT/CT is added at the early, delayed, or both acquisitions. Parathyroid adenomas retain sestamibi longer than normal thyroid tissue, appearing as persistent foci of uptake on delayed images.
Dual-tracer subtraction (sestamibi + pertechnetate or I-123): Sestamibi is taken up by both thyroid and parathyroid tissue, while pertechnetate (or I-123) is taken up only by thyroid. Digital subtraction of the thyroid-only image from the sestamibi image isolates parathyroid uptake. SPECT/CT is then acquired for 3D localization.
Diagnostic performance: Reported sensitivities of sestamibi dual-phase scan with SPECT/CT range from 67% to 86%. A meta-analysis of 24 studies found a pooled sensitivity of 86% for SPECT/CT, compared with 74% for SPECT alone and 70% for planar imaging alone. ]In patients with concomitant thyroid nodular disease, the addition of CT to a dual-tracer SPECT scan increases sensitivity from 80% to 94%. The positive predictive value (PPV) is consistently high, reported at 91–96% across studies.
Limitations: Sensitivity decreases with multigland disease (24–66%), smaller adenomas, and uptake masked by retained radiotracer in adjacent thyroid or submandibular gland tissue.
What is the mechanism by which a SPECT-CT locates parathyroid adenomas?
Mechanism and technique in detail: Tc-99m sestamibi (MIBI) is a lipophilic cation that accumulates in mitochondria-rich tissue in proportion to metabolic activity and blood flow. Parathyroid adenomas, being hypercellular and mitochondria-dense, avidly take up sestamibi and wash it out more slowly than normal thyroid tissue — this differential washout is the basis for detection. The SPECT acquisition provides 3D tomographic data that improves contrast resolution over planar imaging, and the co-registered CT component provides precise anatomic localization, allowing the surgeon to identify the adenoma's relationship to surrounding structures (trachea, esophagus, carotid sheath, mediastinum).
Example of SPECT with localization of a parathyroid adenoma


Axial SPECT showing a right parathyroid adenoma
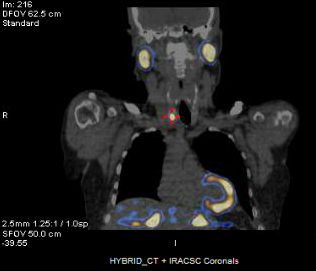
Coronal SPECT showing a right parathyroid adenoma
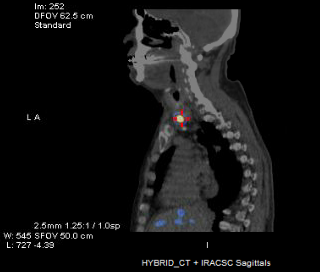
Sagittal SPECT showing a right parathyroid adenoma
This page