Conditions: Head and Neck Tumors (Growths, Lumps, Masses)
Tumors occurring in the mouth, throat, neck, or on the skin may be benign or malignant, but they create a scare either way. A full head and neck evaluation by a head and neck surgeon, including possibly looking in the nose and throat with a scope, and possible biopsy are the first steps that will allow diagnosis. You will have the opportunity to learn about various treatment options, whether surgical or otherwise, before deciding on a course of action.
Neck mass
Because of the wide variety of tissue types within the small space of the neck, the identity of a lump, fullness, or growth in the neck may not be immediately identifiable. Certain history and physical examination findings are very helpful in determining how to further evaluate and manage a neck mass.

Lymph node enlargement
Lymph node enlargement in the neck may simply be the result of inflammation, but persistence, lack of pain, and progressive growth over weeks or months in particular require evaluation for a more serious problem, such as cancer. Differentiating between an enlarged lymph node that is working properly in fighting germs (reactive inflammation), enlarged due to a problem in its functioning (such as with granulomatous disease including sarcoidosis), or containing cancer cells is a common task for the physician. If a lymph node persists for greater than about seven weeks, further evaluation may be necessary, such as examination, imaging and needle biopsy. Cancer in one or more lymph nodes may have spread from a primary cancer elsewhere in the body (such as tonsil cancer spreading to neck lymph nodes), or could represent a type of cancer starting in the lymph nodes (lymphoma).
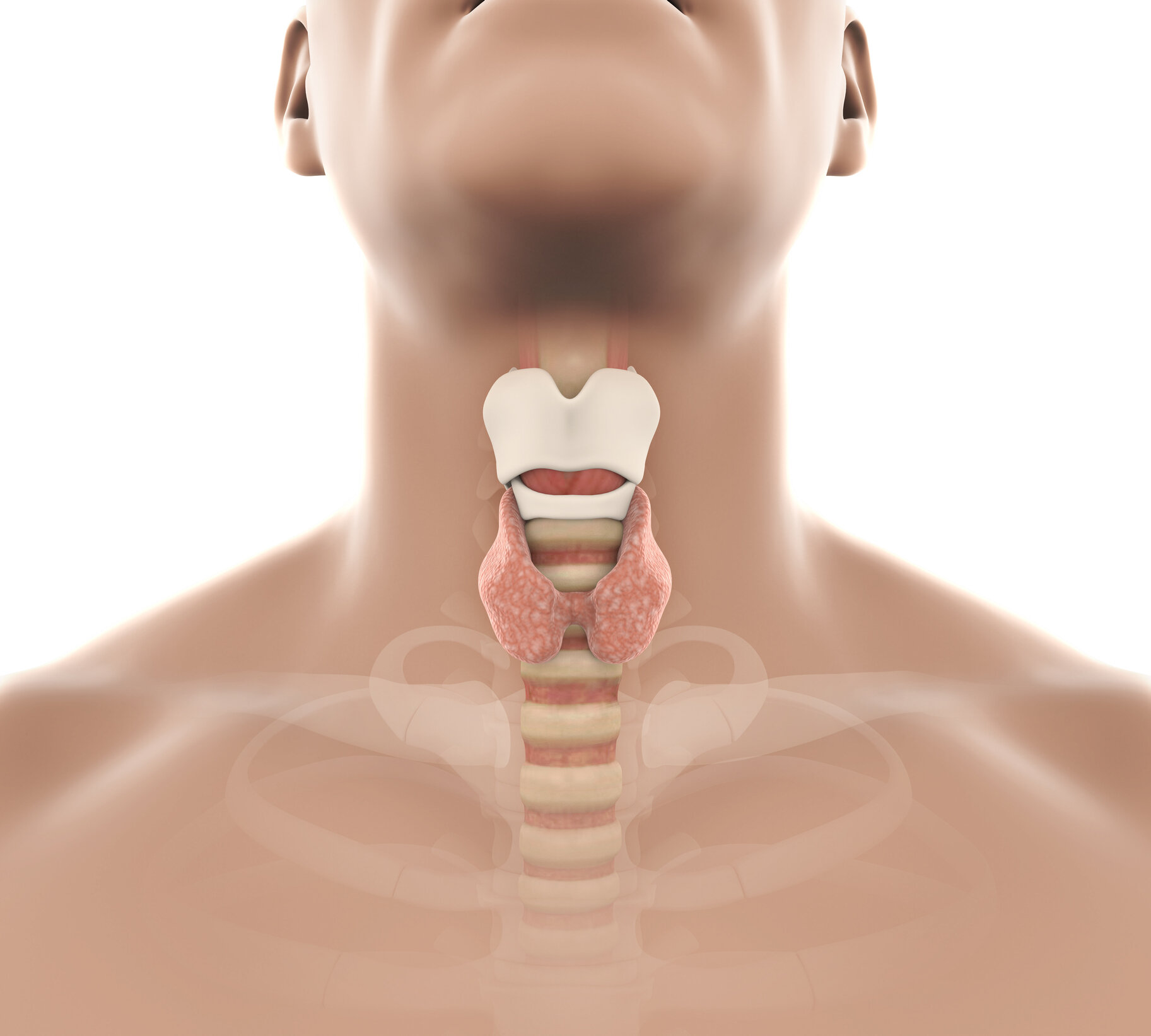

thyroid enlargement and nodules
Located in the midline of the lower neck, the thyroid gland commonly develops lumps or bumps referred to as nodules. The good news is that only one out of 20 nodules are cancerous, the remainder benign. Sorting out which nodules are risky enough to merit a biopsy, and based on those results, determining which subset needs surgery is the usual workup. Papillary thyroid carcinoma, follicular thyroid carcinoma, medullary thyroid carconoma, and anapestic thyroid carcinoma are the categories of thyroid cancer.
Parathyroid adenomas and hyperparathyroidism

The parathyroid glands (which are completely different in function from the adjacent thyroid gland) make parathyroid hormone, which circulates in the blood and maintains a concentration of calcium in the blood. When one or more parathyroid glands becomes “stuck in the on position,” unable to adjust production of parathyroid hormone according to the blood calcium, an insidious condition known as primary hyperparathyroidism exists.


Skin growths
Skin swellings or growths have many causes, including benign and cancerous. Evaluation of new or changing skin growths is necessary to differentiate the dangerous from non-dangerous. Skin cancer is very common, and is the most common type of all cancers. The majority of skin cancers can be treated effectively or “cured” with surgery to remove the cancer, though other types of treatments are utilized in certain circumstances. The specific type of skin cancer generally predicts its behavior, and this information is used to guide treatment. Actinic keratosis, keratoacanthoma, basal cell carcinoma, squamous cell carcinoma, melanoma, and Merkel cell carcinoma are some types skin tumors.
Oral (mouth) tumors


The mouth includes the lips, the teeth, and all other surfaces that would contact a liquid you swish in your mouth. Other than teeth, the surface of the mouth, called mucosa, is a protective covering with glands (for saliva and mucus) within it. Tumors from the mucosa surface include cancers and non-cancers. Among the cancers, squamous cell carcinoma is most common, followed by adenocarcinoma, but may also include melanoma. Non-cancerous growths may include such things as blocked salivary glands, slow-growing boney prominences called tori, viral growths (papillomas), and scars or healing tissue. The roots of teeth can also create tumors, both cancerous and non-cancerous.
Throat (pharynx) tumors

The throat (pharynx) extends from the back of the nose down to the top of the esophagus. This passageway contains various anatomic features, each with different types of tissues, accounting for various predispositions for types of cancers. In other words, certain types of cancer tend to arise more or less in a given anatomic site. The behavior of a cancer in the throat also depends largely on the specific type or subtype of cancer. For example, squamous cell carcinoma of the tonsil that positive for p16 behaves differently from squamous cell carcinoma of the tonsil that is negative for p16. Another example is that cancer of the nasopharynx (located at the top of the throat, behind the nose) acts differently and is therefore treated differently than cancer of a tonsil.
larynx (voice box) tumors

Growths involving the voice box (larynx) range from areas of swelling (such as vocal nodules or vocal cord edema) to papillomas or other benign tumors to malignant (cancerous) tumors. Since the sound produced by the vocal cords may be altered by even small changes in their anatomy, a growth on the vocal cords themselves typically manifests early with hoarseness. In other areas, of the larynx, a growth may become quite large before showing itself by symptoms of difficulty in breathing or swallowing. For these reasons, hoarseness for greater than one month duration, difficulty swallowing or symptoms of blockage of the larynx airway are evaluated by physical exam by a specialist, often including office laryngoscopy—a safe and quick look at the throat and larynx anatomy. Further evaluation may involve biopsy or imaging, such as a neck CT scan. Some of the more common growths on the larynx include squamous papilloma, vocal nodule, and a cancer called squamous cell carcinoma.
branchial cleft cyst

A branchial cleft cyst is another benign condition that can arise at any time, can become infected, and requires definitive diagnosis to differentiate it from cancer. A branchial cleft cyst is a fluid filled swelling in the upper part of the side of the neck. It can, but does not usually have an opening to the skin surface, called a fistula. Branchial cleft cysts account for almost 20% of neck masses in children. Most branchial cleft cysts present in late childhood or early adulthood as a solitary, painless mass, which went previously unnoticed, that has now become infected (typically after an upper respiratory tract infection). A fistula, if present, is asymptomatic until infection arises. A branchial cleft cyst is the remnant of embryonic development and result from a failure of obliteration of one of the branchial clefts, which are homologous to the structures in fish that develop into gills. The diagnosis of branchial cleft cysts is typically made by history and physical exam due to their relatively consistent location in the neck, typically anterior to the sternocleidomastoid muscle. For masses presenting in adulthood, the presumption should be a malignancy until proven otherwise, since carcinomas of the tonsil, tongue base and thyroid may all present as cystic masses of the neck. Unlike a thyroglossal duct cyst, when swallowing, the mass should not move up or down.
lymphoma

Lymphoma is a cancer of the lymph nodes, and this sometimes shows up in the head and neck area, but also commonly in the arm pits or the groin. Persistently enlarged lymph node(s), especially those growing and non-tender are suspicious for some kind of tumor. A lymphoma may also cause fever and/or night sweats. Diagnosis is typically made by biopsy which is then analyzed by a technique called flow cytometry.

Tumor of the parotid salivary gland.

Th three major salivary glands (left to right) sublingual gland, submandibular gland, parotid gland.
salivary gland tumors
We have three paired major salivary glands, the parotid, the submandibular, and the sublingual glands, as well as thousands of minor salivary glands. These can develop into benign or cancerous tumors (neoplasms), which are distinctly different from a swelling due to infection or trauma. Diagnosis of a salivary gland neoplasm is often confirmed with a biopsy, and imaging may be included in the evaluation. Treatment options depend on diagnosis, but generally include observation, medication, and surgery. Salivary gland tumors may be categorized according to the specific gland involved or by the type of tumor (based on appearance under a microscope), which generally predicts its behavior.

thyroglossal duct cyst
A thyroglossal duct cyst can become evident as a lump in the upper neck near midline, deep to the skin. Although they are known to be the most common pediatric mass, they also present in adults with some frequency. It can occur as a result of development as an embryo, when the thyroid gland normally passes from the tongue down to the low neck but occasionally this process leaves a tunnel or sac behind that can fill with fluid later in life. In other words, if present, it is present at birth, but may not show itself until later in life. Characteristically, the mass will elevate with tongue protrusion or swallowing. Infection of a thyroglossal duct cyst can occur, and can cause pain and difficulty breathing. The mass is benign in 99% of cases, and in the 1% that is malignant, the type of cancer is typically either papillary thyroid carcinoma or squamous cell carcinoma.
others
The list above is far from complete. Other types of neck tumors include carotid body tumors, glomus tumors, schwannomas, cancers that have spread to the neck from elsewhere, and others. After physical exam, biopsy is a mainstay in diagnosis, but this is often used in conjunction with radiographic imaging.

How to get the most from your appointment
Appointment time is valuable. Here are some suggestions to get the most of your appointment. This preparation will help you and your doctor maximize efficiency and accuracy, freeing up time for questions and answers.
• Click here to prepare for your face, head, or neck mass or lump appointment.

This page