Conditions: Voice Disorders (Dysphonia)
Most of us depend on our voice as a basis for communication. Many of us depend on our voice for our livelihood as well. And singers go a step further in vocal demands.
How do you know when your voice is not healthy?
You may have a significant voice problem if any of the following are true:
Your voice becomes hoarse or raspy for longer than one month
You lose your ability to hit some high notes when singing
Your voice suddenly sounds deeper
You require more effort to talk
Your throat often feels raw, achy, or strained
You repeatedly clear your throat
How does the larynx work?
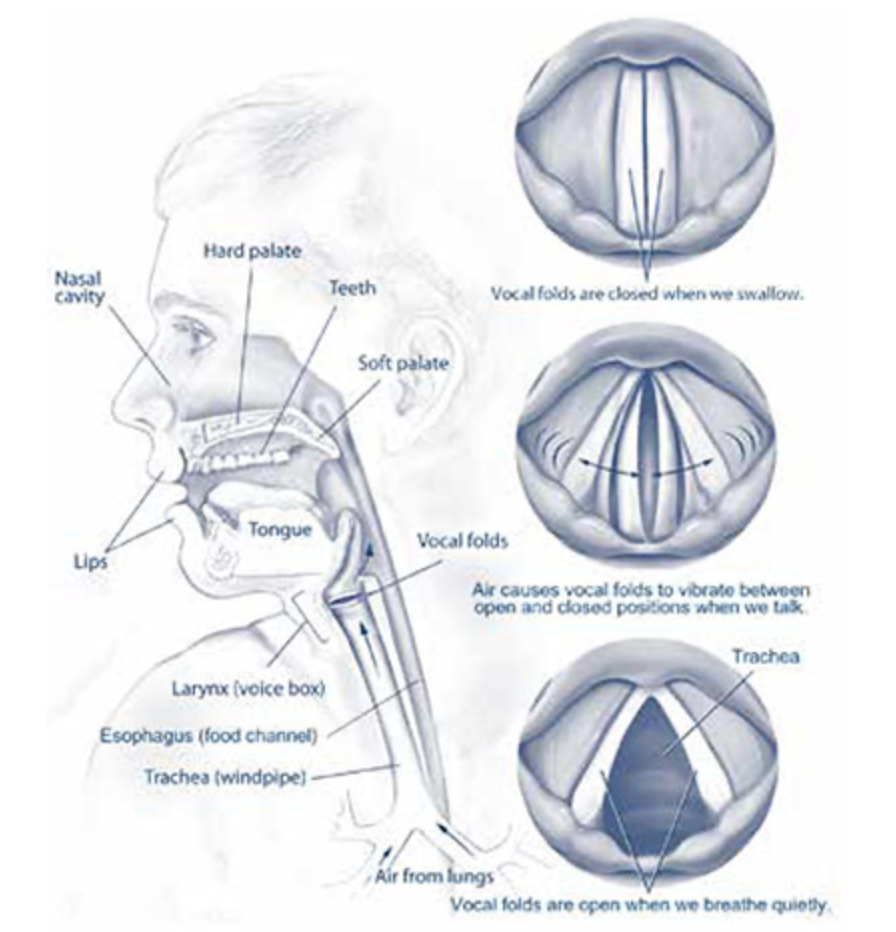
The larynx, also known as the voice box, performs important roles in the generation of sound and speech, in swallowing, and in breathing. Positioned in the neck, specifically between the base of the tongue and the top of the trachea, the larynx consists of various anatomic structures that work harmoniously. When we speak, air expelled from the lungs passes throughthe larynx with the vocal cords closed. Within the larynx, the vocal folds, situated on either side, vibrate against each other as air flows past them, creating sound waves. The pitch of our voice is determined by the tension and length of these folds. As we modulate our voices, muscles within the larynx adjust the position of the vocal folds, altering the pitch, volume, and quality of our speech.
During breathing, the vocal cords open to allow air to pass to and from the lungs.
Additionally, the larynx acts as a crucial guardian of the lower airway, preventing food from entering the trachea and directing it toward the esophagus.

Anatomic sketch with the thyroid removed (dotted line) from the right side view showing anatomy or the right superior laryngeal nerve and the right recurrent laryngeal nerve.
The nerves of the larynx
The nerves of the larynx are the superior laryngeal nerve and the recurrent laryngeal nerve. The superior laryngeal nerve carries sensory fibers to the larynx, while the external branch of this nerve supplies the cricothyroid muscle, responsible for adjusting vocal cord tension during speech, and allowing one to reach a high pitch voice. The recurrent laryngeal nerve controls all of the laryngeal muscles other than the cricothyroid muscle. These muscles move the pieces of the cartilage framework of the larynx for speech, breathing, and swallowing, including the abduction (opening) of the vocal cords for maximal airway and the adduction (closing) of the vocal cords for making noise for speech.
These nerves have a somewhat variable anatomic course from person to person.
Causes of dysphonia (Hoarseness):
The many causes of dysphonia may be categorized into the following groups:
Structural
Neurologic
Functional
Inflammatory
Systemic
These will be elaborated below.
Structural Causes of dysphonia:
Vocal fold lesions (e.g., nodules, polyps, cysts, papillomas, cancer)
Laryngeal trauma or injury
Laryngeal malformations or anatomical abnormalities

Vocal cord lesions
Growths on the vocal cords including nodules, cysts, and tumors can affect the voice because any physical process on the vocal cords can affect the vibrational characteristics of the vocal cord tissue. The size and location of the lesion directly relates to the impact on the voice, with larger lesions or lesions located on the vibrating surface of the vocal cords causing more dysphonia.
Vocal nodules are small, benign growths that develop on the vocal cords, also known as the vocal folds. These nodules are typically caused by excessive or improper use of the voice, such as excessive yelling, singing, or speaking with poor technique.
Vocal cord subepithelial cysts are fluid-filled sacs that develop beneath the surface layer (epithelium) of the vocal cords. These cysts are benign, non-cancerous growths that can form on one or both vocal cords. Subepithelial cysts typically arise from the mucous glands or ducts within the vocal cord tissue. As these structures become blocked or obstructed, fluid accumulates, leading to the formation of a cystic lesion.
Vocal cord papillomas are benign growths that develop on the vocal cords, also known as the vocal folds. These growths are typically small, wart-like lesions that can occur on one or both vocal cords. Vocal cord papillomas are caused by the human papillomavirus (HPV), a common virus that can infect the skin and mucous membranes.
Cancer of the larynx or pre-cancerous lesions such as squamous cell carcinoma in-situ often present first due with dysphonia, especially when the location of the cancer is directly on the vocal cord.
Identification of a growth on the vocal cord visualization of the larynx with use of a scope, usually in a clinic setting. Further testing including videostroboscopy, empiric treatment, or biopsy may be undertaken as needed.
2. Neurological Causes of dysphonia:

The vocal cords move by muscles, and nerves from the brain are the wires that activate these muscles. So, naturally, conditions that affect the nervous system can affect the voice. This can be a vocal tremor, spasmodic dysphonia, vocal cord dysfunction, Parkinson’s disease, and others.
Vocal fold paralysis or paresis
Neurological disorders affecting the larynx (e.g., Parkinson's disease, multiple sclerosis, spasmodic dysphonia)
Neuromuscular disorders, such as myasthenia gravis
3. Functional Causes:
Vocal strain, abuse, or misuse
Muscle tension dysphonia
Vocal Cord Dysfunction / Psychogenic dysphonia

Vocal strain
Hoarseness after yelling at a sports event is just one extreme example of vocal strain. More commonly, people who unknowingly develop habits of using their voice that are harsh on the vocal cords, or people who talk a lot, will develop hoarseness. And when people strain to overcome this hoarseness, the problem worsens, creating a downward cycle.

Muscle tension dysphonia
Muscle tension dysphonia (MTD) is a category of hoarseness (dysphonia) characterized by increased muscle tension of the muscles surrounding the voice box and leading to a breathy or harsh voice. This condition arises as multiple factors (including personal temperament, increased vocal use, and underlying medical or physical causes) cause the muscles of the larynx to become tense. This changes the position of the larynx and affects the cartilaginous structures within the larynx leading to abnormal voice production (phonation). Unlike spasmodic dysphonia (described below), MTD affects all vocal tasks (talking, singing). MTD may be the result of a medical condition (such as reflux, a vocal nodule, and post-menopausal hormone levels) or it may be without identifiable physical cause. Diagnosis is made by an otolaryngologist and/or a speech pathologist. Listening to the voice during different vocal tasks, finding elevation of the thyroid cartilage on palpation and seeing a gap between the vocal cords toward the back of the larynx when viewed with a scope are among the examination findings supporting the diagnosis, helping to differentiate MTD from other dysphonias.
Paradoxical vocal cord movement, also known as paradoxical vocal fold motion (PVFM), is a condition characterized by the abnormal closing of the vocal cords during inhalation, rather than the typical opening. This phenomenon can lead to breathing difficulties, stridor, and a sensation of throat tightness or choking. The underlying causes of PVFM are not fully understood, but it is often associated with various medical conditions, such as asthma, gastroesophageal reflux disease (GERD), and psychological factors like anxiety or stress. Proper diagnosis and management of PVFM typically involve a multidisciplinary approach, including speech therapy, respiratory therapy, and, in some cases, pharmacological interventions or even surgical procedures.
4. Inflammatory Causes:
Laryngitis (acute or chronic)
Reflux laryngitis
Allergic or irritant-induced laryngitis
Laryngitis
Laryngitis, both acute and chronic, can significantly impact an individual's voice. Acute laryngitis, most often caused by a viral infection, can result in a hoarse, raspy, or even complete loss of voice due to inflammation affecting the physical vibrational characteristics of the vocal cords.
Chronic laryngitis, on the other hand, is a persistent inflammation of the larynx, which can be caused by various factors such as acid reflux, overuse of the voice, or exposure to irritants. This long-term condition can lead to a permanently altered voice quality, characterized by a breathy, strained, or low-pitched tone, making communication and vocal performance more difficult.

Reflux
Reflux, or more specifically, laryngopharyngeal reflux, is when stomach acid and digestive enzymes travel up the esophagus and contact the lining of the throat and voice box. While the stomach itself has protection against these caustic liquids, the throat does not, and this commonly affects the voice by inciting inflammation, swelling, and even strategies adopted to compensate for the irritation.

Irritants
Like the skin, the vocal cord surface has only so much defense against irritants. Smoke, reflux from the stomach, and other insults can cause swelling, inflammation, and irregularity to to vocal cord surface, which worsens voice quality.
5. Systemic Causes:
Hormonal imbalances (e.g., hypothyroidism, menopause)
Autoimmune disorders (e.g., Sjögren's syndrome)
Aging-related changes in the larynx

Get the most from your voice appointment
Appointment time is valuable. Here are some suggestions to get the most of your appointment.
This page